Yes, women with PCOS can get pregnant. Polycystic ovary syndrome is the single most common hormonal cause ofinfertility in Indian women, but it is also one of the most treatable. Most women with PCOS conceive after structured lifestyle changes and targeted medical care, ovulation induction with letrozole or clomiphene, IUI, or IVF,where needed.
What is PCOS, and How Common is It in India?
Polycystic ovary syndrome (PCOS) is a hormonal disorder in which the ovaries produce higher-than-usual levels of androgens (male hormones), which disrupts ovulation and the menstrual cycle. Despite the name, ovarian cysts are not required for diagnosis. PCOS typically presents between the late teens and early thirties, often first noticed when a woman tries to conceive.
In India, PCOS prevalence is substantially higher than the global average of 8–13%. A 2024 ICMR national multicentric study of 9,824 women found a weighted prevalence of 19.6% by Rotterdam 2003 criteria. Regional studies in Delhi NCR (2024) report rates of 17.4% among young women aged 18–25, with urban prevalence consistently higher than rural.
Source / Region
PCOS Prevalence
Population Studied
Global (WHO)
8–13%
Reproductive-age women
HibICMR National (2024)
19.6% (Rotterdam)
9,824 women, ages 18–40
Delhi NCR (2024)
17.4%
College-going women, 18–25
Mumbai (urban)
22.5%
Community-based, Rotterdam
South India (adolescents)
~18%
Young adolescent females
Translation for anyone reading this in Delhi NCR: roughly one in five women of reproductive age around you is likely to meet PCOS criteria, though an estimated 70% remain undiagnosed globally. That diagnostic gap is the single biggest obstacle to getting pregnant with PCOS, not the condition itself.
Why PCOS Makes Pregnancy Harder and Why It Doesn't Make It Impossible
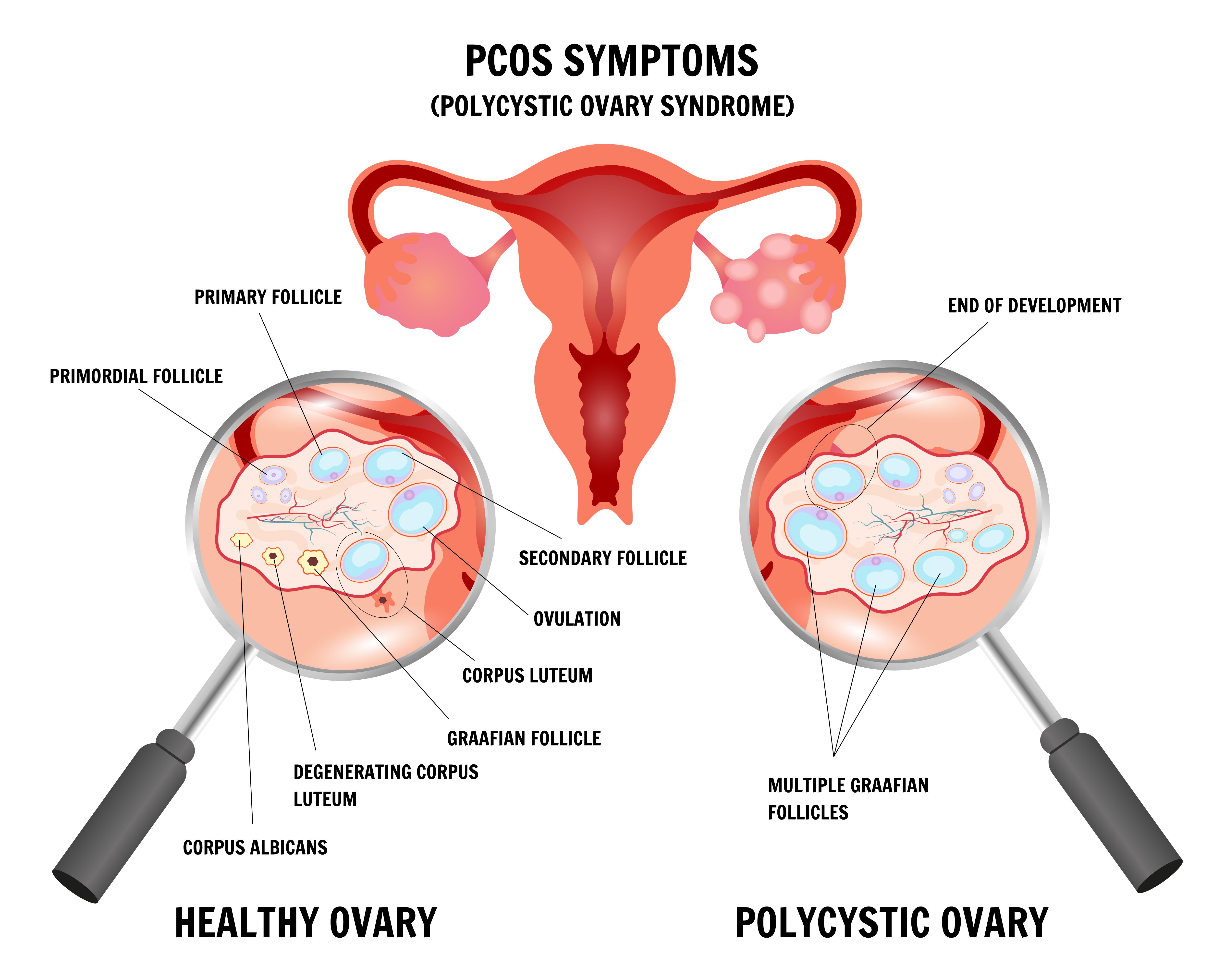
Conception depends on a predictable sequence: a follicle matures, an egg is released (ovulation), it meets sperm in the fallopian tube, and the resulting embryo implants in a receptive uterine lining. PCOS disrupts the first two steps. Elevated androgens and luteinising hormone (LH), combined with insulin resistance, prevent follicles from maturing normally. Many small follicles develop, but none release an egg. Without ovulation, there is no egg for sperm to fertilise.
This is why women with PCOS often experience long cycles (35+ days), skipped periods, or months of unpredictable bleeding. However, PCOS rarely affects egg quality, the uterus, or the fallopian tubes. The ovaries typically hold an above-average reserve of eggs. The problem is almost entirely one of release timing, and release timing is the most treatable variable in fertility medicine. Once ovulation is restored, pregnancy outcomes for women with PCOS are comparable to, and in some IVF studies marginally better than, those of women without PCOS.
Can You Get Pregnant With PCOS? The Step-by-Step Treatment Ladder
Fertility specialists approach PCOS using a graduated treatment ladder. The vast majority of women conceive at the first or second step; only a minority need IVF. The ladder matters because each step has different costs, time commitments, and success rates, and starting at the right rung saves months.
Step 1 Lifestyle Optimisation (First 3–6 Months)
For women with a BMI above 25, a modest weight loss of 5–10% alone restores ovulation in 30–50% of cases. This is not about aggressive dieting; it is about reducing insulin resistance, the metabolic engine behind most PCOS. A structured plan with a dietician, a consistent sleep routine, resistance training combined with cardio, and stress reduction are the foundational layers. Even normal-weight women with PCOS benefit from insulin-sensitising nutrition patterns. Most specialists recommend a 3-month baseline of lifestyle change before adding medication, unless age or diminished ovarian reserve makes time of the essence.
Step 2 Ovulation Induction Medication
When lifestyle alone does not restore cycles, oral medication is the next step. Letrozole is now the international first-line choice for PCOS, having outperformed clomiphene citrate in a landmark randomised trial by Legro and colleagues, with cumulative live birth rates of 28% versus 19% in favour of letrozole. Clomiphene remains widely used, particularly where letrozole is not tolerated. On average, women require about three cycles of ovulation induction to conceive. Metformin, an insulin-sensitising drug, may be added when insulin resistance is prominent. Specific prescriptions, dosages, and duration should be decided with your fertility specialist. These medications require cycle tracking with ultrasound.
Step 3 IUI (Intrauterine Insemination)
If ovulation induction produces eggs but pregnancy does not follow after 3–6 cycles, or if there is a mild male-factor issue or unexplained delay, IUI is the next rung. It pairs ovulation induction with a timed placement of washed sperm directly into the uterus. For PCOS patients, cumulative live birth rates reach around 31% across three IUI cycles, with roughly 98% of successful pregnancies occurring within the first three attempts.
Step 4 IVF (In-vitro Fertilization)
IVF is indicated when oral medications and IUI have not worked, when there is a coexisting factor (tubal disease, significant male-factor infertility, advanced maternal age), or when time is limited. Women with PCOS typically respond well to IVF; their ovaries produce more eggs than average. The trade-off is a higher risk of ovarian hyperstimulation syndrome (OHSS), which is managed by experienced centres through tailored stimulation protocols, GnRH-agonist triggers, and elective freeze-all strategies that transfer the embryo in a later cycle. For women with PCOS under 35, per-cycle clinical pregnancy rates at well-run centres often match or exceed those of age-matched non-PCOS patients.
Why Fertility Differs From One Woman With PCOS to the Next
Two women with the same diagnosis can have very different conception timelines. The factors that drive the difference matter for treatment planning:
• Insulin resistance drives the vast majority of PCOS symptoms in Indian women. Higher insulin levels signal the ovaries to produce more androgens, which suppresses ovulation. Insulin-resistant PCOS is the most responsive to lifestyle change plus metformin.
• Body weight and a BMI above 25 increase time-to-pregnancy and reduce response to ovulation induction. But normal-weight ("lean") PCOS is real and equally treatable; it is often missed on routine check-ups because weight is the first thing clinicians look at.
• Age fertility for PCOS is best in the twenties and early thirties. After 35, egg quality declines begin to compound, and treatment timelines shorten.
• Thyroid status, a coexisting hypothyroid or hyperthyroid state, blocks ovulation independently of PCOS and must be corrected before or alongside fertility treatment.
• The partner's semen parameters, sperm count, and motility in the male partner determine whether IUI or IVF is the right step. A semen analysis is non-negotiable at the first fertility consultation, regardless of how confident the male partner feels.
• The severity of androgen excess, such as severe acne, heavy hirsutism, or very high testosterone, suggests a more androgen-driven phenotype that typically needs medication earlier in the pathway.
What You Can Actually Do Right Now
Before anything else: most PCOS-related infertility is solvable, and the earliest actions are the ones you can take today. These are advisory; they are not a substitute for a fertility evaluation, but they lay the foundation on which every downstream treatment depends.
Lifestyle Foundations (Start This Week)
• Eat for insulin sensitivity: a mostly whole-food, lower-glycaemic-load eating pattern is most effective. That means replacing refined carbohydrates (maida, white rice, sugar) with whole grains, pulses, vegetables, and protein at every meal. Traditional Indian patterns done well, dal, sabzi, dahi, millets, moderate roti fit this model naturally. Work with a dietician rather than following generic internet plans.
• Move regularly: combining resistance training (2–3 times a week) with moderate cardio (30 minutes, most days) reduces insulin resistance faster than either alone. Consistency matters more than intensity. Walking after meals is one of the most underrated interventions.
• Sleep protects ovulation: women who sleep less than six hours or have irregular shift patterns have worse insulin sensitivity and higher androgens. Aim for seven to eight hours and a stable bedtime.
• Manage stress as a fertility variable: chronic stress raises cortisol, which worsens insulin resistance and disrupts the LH/FSH balance. Mindfulness, yoga, therapy, and saying no to over-commitment all count as fertility strategies.
• Ask before starting supplements: discuss with your specialist rather than self-prescribing. Over-the-counter supplement routines can interfere with prescribed medication, interact with thyroid function, or simply waste money.
When to Seek a Fertility Evaluation
Timing is the single most common reason couples lose months they did not need to lose. Ask for a fertility consultation if any of the following apply:
• under 35 and trying for 12 months without success.
• 35 or older and trying for six months without success.
• at any age, if cycles are consistently longer than 35 days, absent, or unpredictable.
• a confirmed PCOS diagnosis and want to plan pregnancy within the next one to two years, a preconception evaluation shortens the path.
• any coexisting condition (thyroid, diabetes, prior miscarriage, endometriosis symptoms).
Our pre-IVF fertility optimisation programme is designed precisely for women with PCOS who want to build the metabolic and hormonal foundations before starting treatment. It combines endocrine workup, dietitian-led nutrition planning, structured exercise guidance, and cycle tracking so that when medical treatment begins, the response is maximised.
When to See a Fertility Specialist: A Decision Table
A gynaecologist manages PCOS symptoms; a fertility specialist (reproductive endocrinologist) manages the path to pregnancy. The difference matters when time and treatment sequencing are on the line.
Situation
Who to See
Timeline
PCOS symptoms, not trying yet
Gynaecologist/endocrinologist
At diagnosis
Under 35, trying >12 months
Fertility specialist
Book now
35+, trying > 6 months
Fertility specialist
Book now
Mumbai (urban)
Fertility specialist
Within 1–2 months
Prior miscarriage + PCOS
Fertility + high-risk obstetrician
Before the next attempt
Planning pregnancy in 6–12 months
Preconception fertility consult
3–6 months before
If you are in Gurgaon or Delhi NCR, booking a fertility consultation does not commit you to treatment. It establishes baseline hormone levels (AMH, FSH, LH, testosterone, TSH, prolactin), assesses your partner's semen parameters, and gives you a realistic timeline. Most couples leave the first consultation with a clearer plan and significantly less anxiety.
What the Numbers Actually Say: PCOS Fertility Outcomes
Outcome data helps set realistic expectations. The figures below reflect published evidence from international and Indian studies in women under 35 at experienced centres. Individual results depend on age, BMI, duration of infertility, and coexisting factors.
Treatment Step
Pregnancy Rate
Notes
Lifestyle change (5–10% weight loss
30–50% resume ovulation
Over 3–6 months
Letrozole ovulation induction
41% cumulative PR; 28% live birth (Legro RCT)
Historical first-line
IUI (3 cycles, PCOS cohort)
~38% cumulative clinical pregnancy; ~31% live birth
98% of successes in first 3 cycles
IVF PCOS vs. controls (first cycle)
Clinical pregnancy 70.9% vs. 59.8%; live birth 58.3% vs. 52.1%
7,678 patients, retrospective cohort
IVF women with PCOS ≥ 35
Cumulative live birth 55.5% over 2 years
vs. 38% in age-matched controls
The headline: women with PCOS, treated properly, do at least as well as women without PCOS at every rung of the ladder. The increased risks of miscarriage (roughly 1.4× higher) and ovarian hyperstimulation syndrome during IVF are both manageable with experienced care and appropriate protocols (freeze-all cycles, GnRH-agonist triggers, metformin adjuncts where indicated)
Want to consult the best fertility in india? Please find the links below.
Not negatively. Large studies consistently show that women with PCOS achieve clinical pregnancy and live birth rates comparable to and sometimes higher than those of age-matched women without PCOS, because they produce more eggs per cycle.
How long does it take to get pregnant with PCOS?
It varies widely. Some women conceive within three to six months of starting lifestyle change and ovulation induction; others need 12–18 months and may move to IUI or IVF. The strongest predictor is how quickly the right treatment step is reached; delays usually come from late diagnosis, not from PCOS itself.
Is PCOS permanent? Will it go away after I have a baby?
PCOS is a lifelong hormonal and metabolic condition rather than a curable disease, but symptoms often ease after menopause, and pregnancy itself can temporarily reset some metabolic patterns. Lifestyle changes and monitoring remain important across your whole life.
Can I get pregnant naturally with PCOS without any medication?
Yes, many women do, particularly those with milder phenotypes or those who respond strongly to lifestyle and weight changes. Around 30–50% of overweight women with PCOS resume ovulation with a 5–10% reduction in body weight. If you are under 35 with regular enough cycles, a structured 3–6 month lifestyle-first trial is reasonable before considering medication.
Schedule your consultation Today!
Book your consultation with our fertility experts the first step toward your parenthood journey.