
A semen analysis is a laboratory test that measures sperm count, motility (movement), morphology (shape), volume, and other markers of male fertility. According to the WHO 2021 reference values, normal results include a sperm concentration of at least 16 million per millilitre and total motility of 42 per cent or higher. Abnormal results rarely mean the only path forward is IVF.
.jpg)
A semen analysis (often called a sperm test or seminogram) is the first investigation requested when a couple has been trying to conceive for 12 months without success, or 6 months if the female partner is over 35. The test evaluates several parameters in a single ejaculated sample, comparing each against the World Health Organization (WHO) 2021 reference values. These thresholds represent the lower 5th per centile of fertile men whose partners conceived within 12 months. Falling below a reference value does not confirm infertility; it indicates further evaluation is warranted.
Male factors contribute to roughly half of all infertility cases worldwide, yet the workup often focuses on the female partner first. A semen analysis is non-invasive, inexpensive, and frequently the single most informative test in a fertility evaluation. In Indian clinical practice, where male factor remains underdiagnosed, the sample provides a baseline that shapes every subsequent decision: whether to investigate hormonal causes, check for varicocele (enlarged scrotal veins), recommend lifestyle changes, or move directly to assisted reproduction. Two abnormal samples taken at least two to three weeks apart are usually needed before concluding, because sperm production is sensitive to recent illness, fever, stress, and heat exposure. A single below-range result is rarely the final word.
Most reports are organised into three sections: macroscopic findings (volume, colour, viscosity, pH), microscopic findings (count, motility, morphology, vitality), and additional observations such as round cells or agglutination. Reading the report in this order helps you spot whether issues are sample-related, production-related, or transport-related.
Volume below 1.4 mL (hypospermia) can suggest a collection problem, retrograde ejaculation, or a blockage in the ejaculatory ducts. Colour should be grey-white to slightly yellow; red or brown tints may indicate blood and warrant follow-up. pH below 7.2, alongside low volume, points toward seminal vesicle obstruction, while a higher pH may suggest infection.
Concentration is reported as millions per millilitre. Total sperm number multiplies concentration by volume. Both values matter: a high concentration in a tiny volume can still mean a low total count. Common findings include oligozoospermia (low count, below 16 million/mL), severe oligozoospermia (below 5 million/mL), cryptozoospermia (sperm seen only after centrifugation), and azoospermia (no sperm in the sample). Each requires a different next step, which is why isolated numbers must be interpreted alongside hormonal and physical evaluation.
Motility tells you how many sperm are moving. Progressive motility is the more important factor for natural conception because only forward-moving sperm can travel up the female reproductive tract. The WHO 2021 cut-off is 30 per cent progressive motility. Some Indian labs still report the older grade-based system: Grade A (rapid progressive), Grade B (slow progressive), Grade C (non-progressive), and Grade D (immotile). Newer reports combine A and B as progressive motility. Asthenozoospermia (low motility) often improves with lifestyle adjustment, treatment of varicocele, or correction of underlying infection.
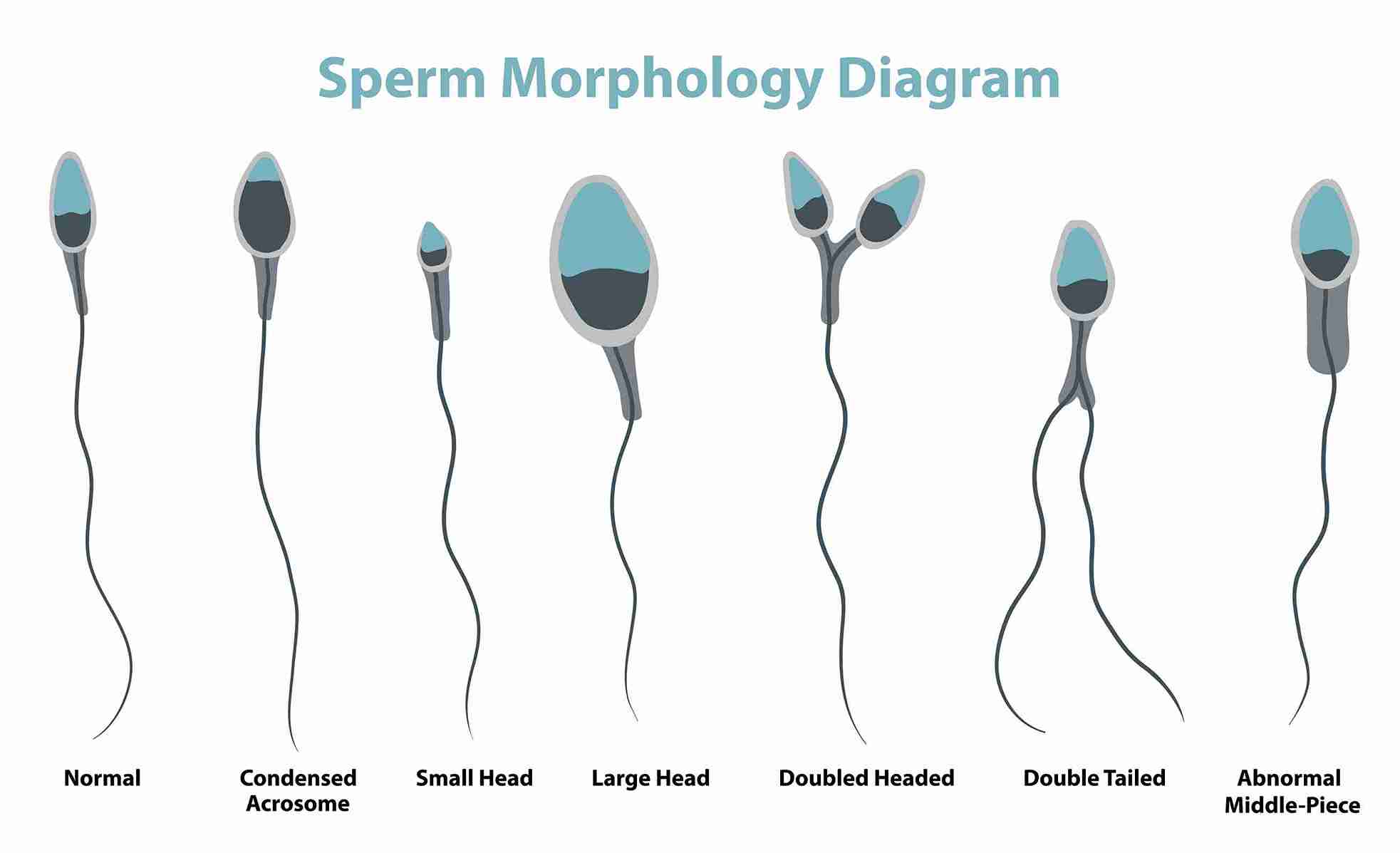
Morphology assesses sperm shape under high magnification. The Kruger strict criteria require at least 4 per cent normal forms. Below this threshold (teratozoospermia) does not mean conception is impossible; many men with 1 to 3 per cent normal forms father children naturally. However, when combined with low count or low motility (oligoasthenoteratozoospermia), the chance of natural conception drops, and assisted reproduction may be discussed.
Elevated round cells (above 1 million/mL) may indicate white blood cells and suggest infection or inflammation. Agglutination (sperm sticking together) can hint at antisperm antibodies, which a MAR test (mixed antiglobulin reaction) confirms. These findings often respond to short courses of treatment under specialist guidance.
Sperm production is influenced by hormonal, anatomical, lifestyle, and environmental factors. Many causes are reversible. Common contributors include:
• Varicocele enlarged veins in the scrotum: with one testicle warmer than the other and visible vein engorgement; treatable surgically when significant.
• Hormonal imbalance, low testosterone, high prolactin, thyroid dysfunction, or pituitary issues that alter the signals driving sperm production.
• Genetic factors, such as Y-chromosome microdeletions, Klystron microdeletions, or chromosomal anomalies, affect around 15 per cent of men with azoospermia.
• Past medical history includes childhood mumps, undescended testes, prior chemotherapy, or scrotal trauma.
• Heat exposure from sauna use, hot baths, prolonged laptop use, or jobs involving high temperatures can all of which can suppress sperm production temporarily.
• Lifestyle factors include smoking, heavy alcohol use, recreational drugs, anabolic steroid use, obesity, and chronic stress.
• Environmental exposure to pesticides, heavy metals, and certain industrial chemicals.
• Infections, untreated urinary tract or sexually transmitted infections, can damage sperm or block ducts.
• Acute illness, recent fever, or systemic illness in the 90 days before the test, since sperm take roughly three months to mature.

The good news is that sperm regenerate roughly every 64 to 72 days, so improvements made today often show up in a repeat test about three months later. Two areas usually deliver the biggest gains: lifestyle changes and targeted medical evaluation.
Lifestyle has a measurable impact on sperm parameters. Stop smoking entirely; tobacco lowers count and motility and increases DNA fragmentation. Limit alcohol and avoid recreational drugs. Bring body mass index into a healthy range, as both underweight and obesity are associated with poorer semen quality. Build regular moderate exercise into the week, but avoid extreme endurance training, which can suppress hormone levels. Manage stress through sleep hygiene, breathing practice, or counselling where useful. Cool the scrotal area: choose looser underwear, avoid prolonged hot baths and saunas, and keep laptops off the lap. A diet rich in leafy greens, berries, nuts, fish, and whole grains supplies the antioxidants and micronutrients that support sperm health. A Cloudnine specialist can advise whether supplementation is appropriate in your case rather than relying on generic over-the-counter products.
Some causes need clinical care, not just lifestyle adjustment. Clinically significant varicoceles respond well to outpatient surgical correction, with semen parameters often improving within three to six months. Hormonal imbalances may be corrected once identified through blood tests for FSH, LH, testosterone, prolactin, and thyroid function. Infections diagnosed through cultures are treated under specialist supervision. For severe male factor infertility, very low count, very low motility, or azoospermia, assisted reproduction techniques such as IUI, IVF, ICSI (intracytoplasmic sperm injection), or surgical sperm retrieval (TESA, PESA, micro-TESE) offer effective routes to parenthood. The choice depends on the underlying cause, the female partner's evaluation, and your shared goals.
Not every abnormal report requires immediate intervention, but some patterns should prompt a specialist consultation rather than a wait-and-watch approach.
If your report shows two abnormal results or you have been trying to conceive for over a year, you can book a fertility consultation at a Cloudnine Fertility centre near you for a complete evaluation.

Outcomes vary widely depending on the cause, the female partner's age and fertility, and the chosen treatment. The figures below summarise published clinical ranges and are intended as a general guide, not a prediction for any individual.