
OHSS (ovarian hyperstimulation syndrome) is an over-response to the fertility medications used in IVF, in which the ovaries swell and leak fluid into the abdomen. Mild forms are common; moderate-to-severe OHSS affects roughly 1-5% of IVF cycles. Call your clinic urgently if you have rapid weight gain, severe bloating, breathlessness, or reduced urination - severe OHSS is a medical emergency.
Ovarian hyperstimulation syndrome is an exaggerated reaction to the injectable hormones used to grow multiple eggs during an IVF (In-vitro Fertilization) cycle. In a normal cycle, one egg matures; in IVF, stimulation encourages many follicles to develop at once. In OHSS, the ovaries become enlarged and release substances that make small blood vessels “leaky”, so fluid shifts out of the bloodstream and collects in the abdomen - and, in severe cases, around the lungs. This fluid shift is what drives the bloating, weight gain and rarely, the breathing and circulation problems that make severe OHSS dangerous.
It is graded by how much it affects you, from mild discomfort that settles on its own to a small number of severe cases needing hospital care. The quick reference below sets out that spectrum; the section that follows explains how to tell the grades apart in real life.
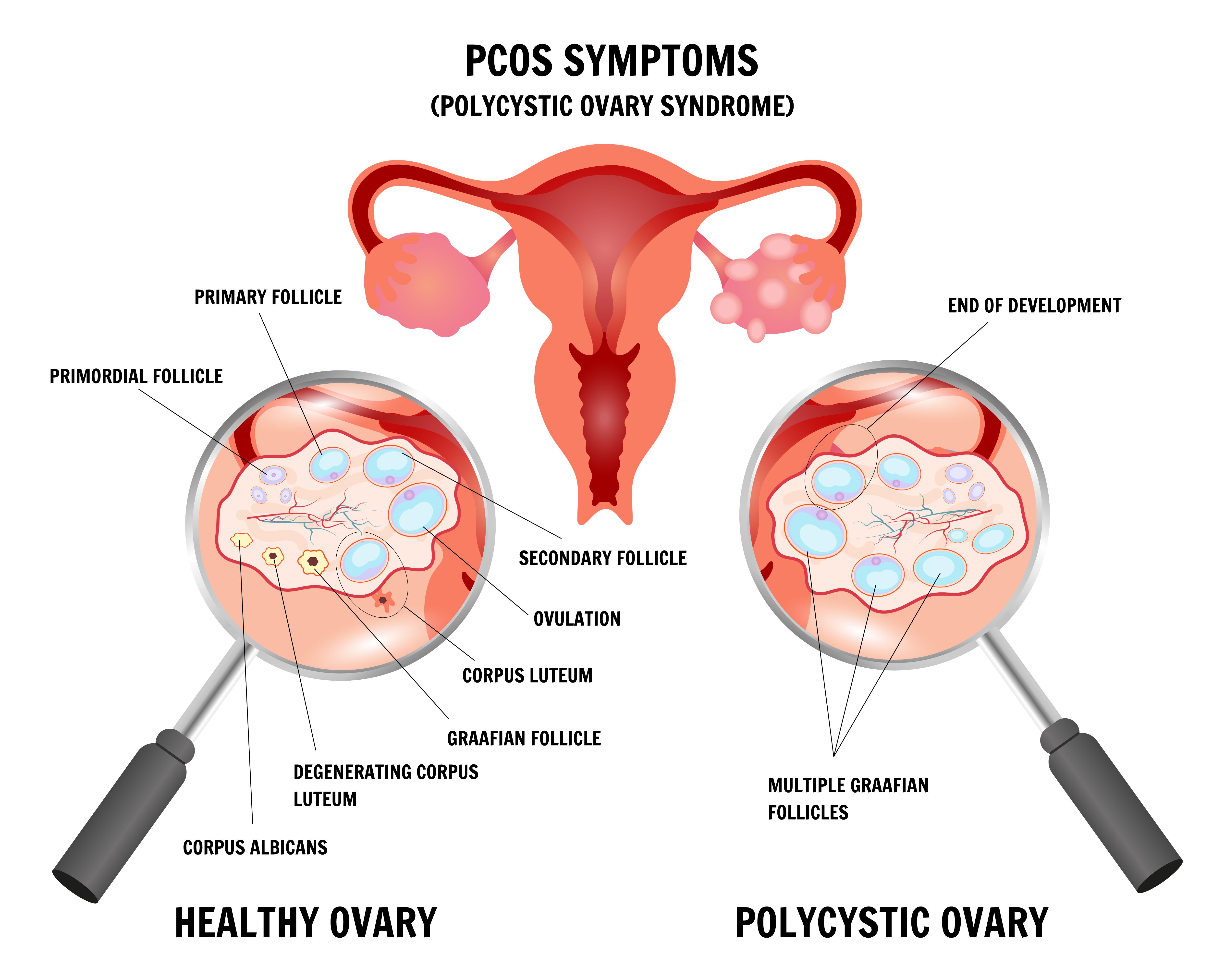
Two of the strongest risk factors for OHSS - being under 35 and having polycystic ovary syndrome (PCOS, a hormonal condition with many small follicles) - are common among women starting IVF in India. PCOS is widely reported in Indian women of reproductive age, and a large proportion of fertility patients here are in their late twenties and early thirties with a high ovarian reserve. A high reserve usually indicates good egg yield, which is encouraging, but it also means the ovaries can overrespond if stimulation is not carefully tailored.
The practical takeaway is reassuring rather than alarming: OHSS is largely predictable and increasingly preventable. A Cloudnine fertility specialist screens for these risk factors before stimulation begins and adjusts the protocol accordingly. What matters most to you as a patient is knowing the warning signs, what to monitor at home, and exactly when to pick up the phone. The rest of this guide is built around those three things.
Most people who develop OHSS have the mild form, which feels like an exaggerated version of normal post-retrieval bloating and eases over a week or so. The skill is recognising when symptoms cross from “uncomfortable but expected” into territory that needs medical input. The grades differ less in which symptoms appear and more in how intense they are, how fast they change, and whether they start affecting your breathing, urine output, or general well-being.
Both - and the timing tells your specialist something important. Doctors describe two patterns. Early OHSS appears within about nine days of the trigger injection (the final injection given before egg collection) and is driven by that injection. Late OHSS starts later, usually after an embryo transfer that has led to pregnancy, because the rising pregnancy hormone keeps the ovaries stimulated. Late OHSS tends to last longer because the hormonal drive does not switch off as quickly. This is precisely why many clinics now freeze all embryos in higher-risk cycles and transfer them later, once the ovaries have settled - it removes the pregnancy hormone surge from the equation during the riskiest window.
Some bloating, tenderness, and a heavy feeling in the lower abdomen are normal for a few days after egg collection, because the ovaries are temporarily enlarged. The features that point towards OHSS rather than ordinary recovery are the ones that escalate rather than settle: swelling that keeps increasing, weight that climbs day on day, breathlessness, and urine output that drops. As a rule of thumb, recovery discomfort plateaus and then improves, whereas OHSS tends to build. If you are five days out from retrieval and feel more bloated and breathless than the day before - not less - that change in direction is the signal to contact your clinic rather than wait.
OHSS begins with an over-vigorous ovarian response to stimulation. The enlarged ovaries release a signalling protein called VEGF (vascular endothelial growth factor), which makes nearby blood vessels leak fluid into the abdomen. The trigger injection - and, in late OHSS, the body’s own pregnancy hormone - is the spark that sets this off. Certain factors make an over-response more likely:
If you suspect OHSS, the priorities are simple: monitor a few specific things at home, support your body with the right fluids, and stay in close contact with your clinic. Self-monitoring is not about diagnosing yourself - it is about giving your specialist objective numbers and catching any worsening early.
This is one of the most common questions, and “just drink lots of water” is poor advice. In OHSS, fluid is leaking out of the blood vessels, so drinking large volumes of plain water alone can dilute the body’s salts and actually make you feel worse. Electrolyte-containing fluids are the better choice: oral rehydration solution (ORS) or culturally familiar options such as coconut water and lightly salted lime water help maintain the salt balance your body needs. Including protein-rich foods in your diet also supports fluid balance. The aim is steady, sensible hydration guided by thirst and urine output - not forcing fluids - and your Cloudnine specialist can give you a target suited to your situation. If you cannot keep fluids down at all, that itself is a reason to be seen.

Use the table below to decide how quickly to act. The left column lists symptoms to report to your clinic the same day; the right column lists symptoms that mean you should seek emergency hospital care without waiting.
Severe OHSS can occasionally cause blood clots and is treated as an emergency for that reason. If you are unsure which column you are in, treat it as the more urgent one and book a fertility consultation or call your clinic’s helpline - it is always reasonable to check.
For the great majority of patients, OHSS is self-limiting and leaves no lasting harm. The ovaries return to their normal size, and outcomes are generally excellent once the episode has resolved. Two questions come up constantly: how long it lasts, and whether it affects the pregnancy. The table summarises the typical picture.
