Poor sperm morphology, where a high proportion of sperm have an abnormal shape, does reduce the chances of natural conception, but it does not make pregnancy impossible. Even men with very low morphology scores can father children, particularly with medical support. The key factors are how low the result is, what is causing it, and whether other sperm parameters, such as count and movement, are also affected.
What is sperm morphology?
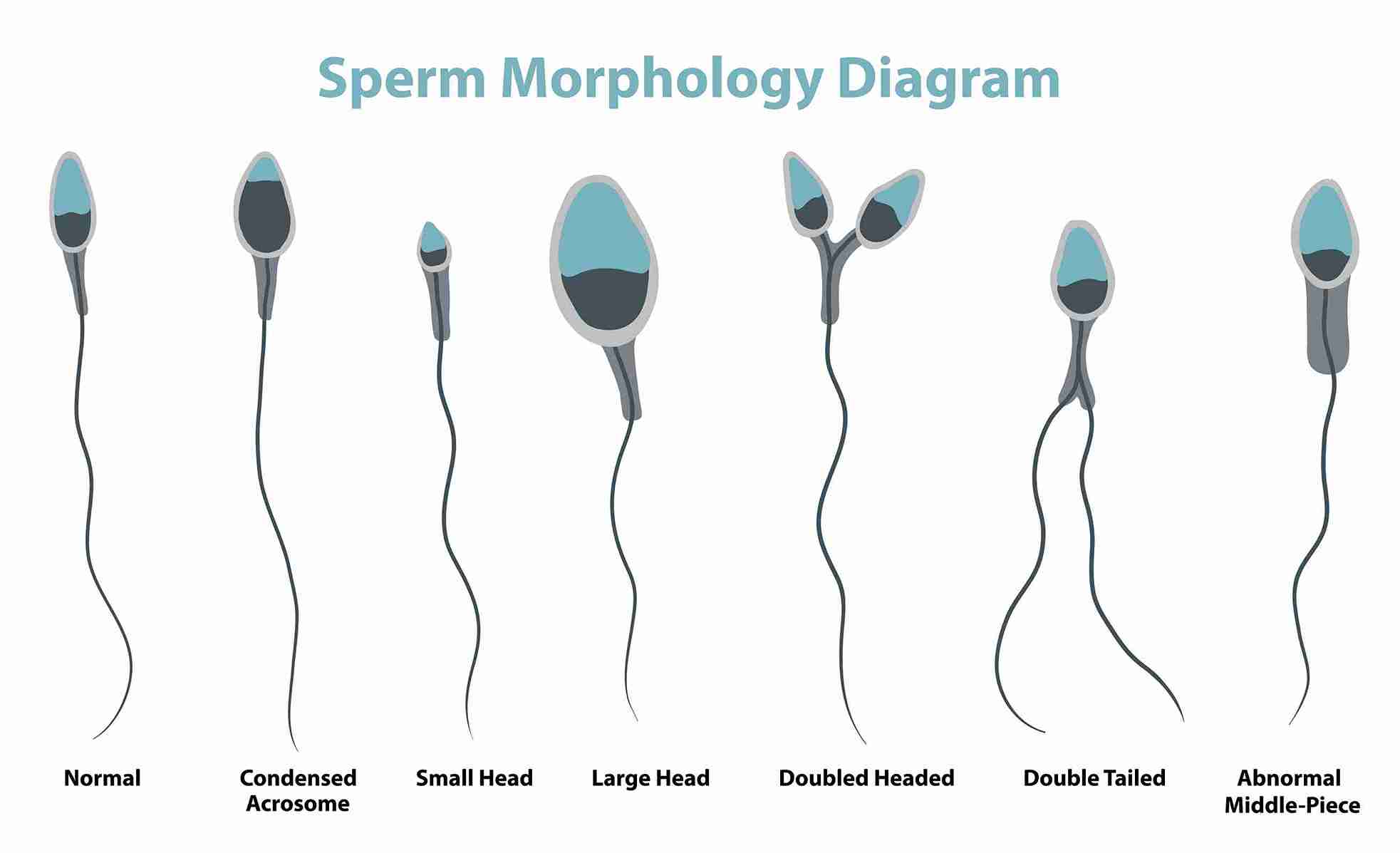
Sperm morphology refers to the size, shape, and structure of sperm cells. A normal sperm has an oval-shaped head, a midpiece that provides energy for movement, and a long tail that propels it forward. Abnormal morphology means a sperm is misshapen in one or more of these areas: a large or irregular head, a bent tail, or a missing midpiece, which makes it harder for the sperm to swim efficiently and penetrate an egg. Morphology is assessed during a semen analysis, where a laboratory technician examines a sample of sperm under a microscope using a standardised scoring system called Kruger Strict Criteria.
Morphology result
Normal forms (%)
What it means
Fertility impact
Normal
≥4% (WHO 2021 standard)
Acceptable proportion of healthy sperm
Natural conception likely possible
Borderline
3–4%
Just below the normal threshold
May take longer; IUI may help
Low (teratozoospermia)
1–3%
Most sperm are abnormally shaped
Reduced natural conception; ICSI recommended
Very low
Below 1%
Severely abnormal morphology
ICSI with specialist review required
Why sperm morphology matters and why it is only part of the picture
When a man receives a semen analysis report showing low morphology, the natural response is alarm. But morphology is one of three key measures in a semen analysis, the other two being sperm count (how many sperm are present) and motility (how well the sperm move). A man with low morphology but a healthy count and strong movement still has a reasonable chance of natural conception, because a large enough number of well-moving sperm will compensate for the proportion that are poorly shaped. In India, stress, heat exposure, and lifestyle factors, including frequent use of hot water baths, laptop heat, and long sedentary work hours, are among the most common and correctable contributors to abnormal morphology. A single test result does not tell the whole story; what matters is the overall picture across all parameters.
How sperm morphology affects the ability to conceive
The relationship between morphology and fertility is not linear. Even at low percentages, conception is possible; the question is how much more difficult it becomes, and through which pathway.
Natural conception with low morphology
Natural conception is still possible with morphology between 1–4%, particularly if sperm count and motility are normal. Because a typical ejaculate contains tens of millions of sperm, even 3–4% normal forms represents hundreds of thousands of correctly shaped sperm reaching the egg. Studies show that couples where the male partner has borderline morphology (3–4%) take on average two to three times longer to conceive naturally compared to couples with normal morphology, but many do conceive without medical intervention. Below 1%, natural conception becomes unlikely, and medical treatment is usually recommended.
How abnormal shape prevent fertilisation
A sperm's shape is not just cosmetic; it directly determines function. Sperm with abnormal heads struggle to bind to and penetrate the egg's outer layer. Sperm with bent or missing tails cannot generate the movement needed to reach the egg in the first place. Sperm with midpiece defects lack the energy to sustain their journey through the female reproductive tract. This is why morphology matters even when counts are high; a large number of poorly functioning sperm is less useful than a smaller number of well-formed ones.
Morphology and IVF success rates
During standard IVF, in which sperm and eggs are placed in a dish, and fertilisation occurs naturally, low egg morphology reduces the fertilisation rate. This is why most fertility clinics in India recommend moving directly to ICSI (intracytoplasmic sperm injection, a technique where a single selected sperm is injected directly into the egg) for men with morphology below 4%. ICSI bypasses the need for sperm to penetrate the egg on its own, largely removing morphology as a barrier to fertilisation. ICSI success rates at Cloudnine Fertility are not significantly lower in men with low morphology than in those with normal morphology, provided egg quality is good.
Does morphology affect the health of the baby?
This is one of the most common questions men ask after receiving a low morphology result. The current medical evidence is reassuring: abnormally shaped sperm rarely carry the genetic material needed to fertilise an egg, so they are naturally filtered out during conception. The sperm that does fertilise the egg is, by definition, one that was capable of doing so. There is no evidence that low morphology in itself increases the risk of birth defects or chromosomal problems in children conceived naturally or through ICSI.
What causes abnormal sperm morphology?
Sperm morphology is affected by conditions that disrupt the normal process of sperm production, which takes approximately 72 days in the testicles. The most common causes include:
Heat exposure: Testicles function best at 2–3 degrees below core body temperature, and prolonged heat from laptops, hot water baths, or tight clothing raises scrotal temperature, directly damaging sperm structure during development.
Varicocele: An enlargement of the veins inside the scrotum, present in roughly 15% of all men and up to 40% of men investigated for infertility, raises testicular temperature and creates a hormonal environment that impairs normal sperm formation.
Infections: Sexually transmitted infections such as chlamydia or gonorrhoea, and other reproductive tract infections, can cause inflammation that damages the cells responsible for producing normally shaped sperm.
Oxidative stress: Smoking, heavy alcohol consumption, and exposure to environmental pollutants generate harmful molecules called free radicals that damage the sperm's genetic material and outer structure, leading to abnormal shapes.
Hormonal imbalance: Low testosterone or high levels of other hormones, such as prolactin (a hormone produced by the pituitary gland in the brain), disrupt the chemical signals that control sperm development.
Genetic factors: Some men have inherited conditions that affect sperm production at a structural level, resulting in consistently abnormal morphology that does not respond to lifestyle changes.
Certain medications: Long-term use of anabolic steroids, some antibiotics, and chemotherapy drugs can impair sperm production and distort sperm shape, sometimes temporarily and sometimes permanently.
Reduce heat exposure immediately: Stop using a laptop on your lap, switch from hot to warm water baths, and avoid long sauna or steam room sessions. Sperm take 72 days to mature, so changes made now will show in test results roughly two to three months later.
Quit smoking and limit alcohol: Smoking has a direct, dose-dependent effect on sperm morphology; the more cigarettes smoked per day, the greater the impact. Even cutting down significantly improves results over 2–3 months.
Take antioxidant supplements: Vitamins C and E, zinc, selenium, and coenzyme Q10 have evidence supporting their ability to reduce free-radical damage that distorts sperm shape. A daily male fertility supplement containing these (available at Indian pharmacies for ₹500–₹1,500/month) is a reasonable starting point.
Eat a diet rich in folate and zinc: Green leafy vegetables, lentils, pumpkin seeds, and chickpeas provide the micronutrients most directly linked to normal sperm production, particularly relevant for vegetarian Indian diets.
Maintain a healthy weight: Excess body fat, particularly around the abdomen, raises estrogen levels in men and lowers testosterone, both of which negatively affect sperm shape and count.
Medical and clinical treatments
Varicocele repair: If a varicocele is identified on ultrasound, surgical repair (varicocelectomy) significantly improves sperm morphology in around 60% of men within 3–6 months one of the most effective treatments available.
Antioxidant therapy prescribed by a specialist: A fertility doctor can prescribe higher-dose antioxidant regimens and monitor their effect on morphology through follow-up semen analyses every 3 months.
Treat underlying infections or hormonal issues: Infections and hormonal imbalances causing abnormal morphology respond well to targeted medical treatment, often restoring normal values within one to two sperm production cycles (approximately 3–6 months).
ICSI (Intracytoplasmic Sperm Injection): For men with morphology below 4%, or where lifestyle changes have not improved results sufficiently, ICSI is the recommended fertility treatment. A single healthy sperm is selected and injected directly into an egg, bypassing the need for the sperm to penetrate the egg on its own.
When to see a fertility specialist
A single semen analysis showing low morphology is not necessarily a reason for immediate medical intervention; lifestyle changes alone can produce meaningful improvement in many cases. However, the following situations warrant an early specialist consultation rather than waiting:
Your situation
What it may indicate
Recommended action
Morphology below 1%
Severe teratozoospermia
Specialist review + ICSI assessment
Low morphology + low count or poor motility
Multiple sperm parameter issues
Immediate specialist referral
Trying to conceive for 12+ months (under 35)
Clinical infertility definition met
Full fertility evaluation for both partners
Trying for 6+ months (over 35)
Age-related urgency
Specialist consultation without delay
Lifestyle changes for 3+ months with no improvement
Possible structural or genetic cause
Further investigation of genetic or hormonal
Pain, swelling, or prominent veins in the scrotum
Possible varicocele
Scrotal ultrasound + surgical review if confirmed
Cloudnine Fertility's male fertility specialists in Bangalore, Delhi, Mumbai, Hyderabad, Chennai, and Pune offer a comprehensive semen analysis, hormonal assessment, and personalised treatment plan, including varicocele evaluation and ICSI planning where needed. Book a male fertility assessment at your nearest centre.
What the research says: morphology and treatment outcomes
Clinical studies consistently show that morphology alone is a poor predictor of IVF or ICSI outcome when other parameters are normal. The figures below reflect published evidence and Indian fertility clinic data:
Scenario
Outcome
Source
Varicocele repair in men with low morphology
60% show meaningful morphology improvement within 6 months
Asian Journal of Andrology, 2021
ICSI with morphology below 4%
Fertilisation rate not significantly different from normal morphology
Human Reproduction Update, 2020
Antioxidant supplementation (3 months)
Average 1–2% improvement in normal forms
Andrology, 2019
Couples with borderline morphology (3–4%) are trying naturally
~70% conceive within 2 years without treatment
Fertility & Sterility, 2018
If your semen analysis has flagged low morphology and you are unsure of the next step, Cloudnine Fertility's male fertility specialists in Bangalore, Delhi, Mumbai, Hyderabad, Chennai, and Pune can help you understand your results, identify the cause, and put a clear treatment plan in place, whether that means lifestyle support, varicocele assessment, or ICSI planning. Book your male fertility consultation today.