Embryo cryopreservation is the procedure of freezing IVF (In-vitro Fertilization) embryos for future use. At Cloudnine Fertility, embryos are typically frozen at the blastocyst stage using vitrification (ultra-rapid freezing) and stored in liquid nitrogen at -196 °C. The process protects embryo quality, allows safer single-embryo transfers, and is fully permitted under Indian law.
Embryo cryopreservation is the laboratory technique of cooling fertilised IVF embryos to sub-zero temperatures so that all biological activity pauses, the embryo remains viable for years, and it can later be thawed and transferred into the uterus. Modern fertility centres use vitrification - a rapid-cooling method that turns the embryo into a glass-like state without forming damaging ice crystals - rather than the older slow-freezing approach. The result is markedly higher post-thaw embryo survival, often above 95% at Cloudnine Fertility-grade laboratories.

Two decades ago, embryo freezing in India was a backup plan; today it is part of the main treatment pathway in most well-equipped fertility centres in Gurgaon, Delhi NCR, and other metros. Three shifts have driven this. First, vitrification replaced slow freezing in the mid-2000s and dramatically improved post-thaw survival. Second, growing evidence suggests that frozen embryo transfer can offer comparable, and in some patient groups slightly better, live birth rates compared with fresh transfer, while reducing the risk of ovarian hyperstimulation syndrome (OHSS). Third, the Assisted Reproductive Technology (Regulation) Act, 2021 - the ART Act - gave embryo freezing in India a clear legal framework. The result is that most IVF cycles at a Cloudnine Fertility-grade centre now involve at least some embryo freezing as standard.
Embryo cryopreservation is layered onto an existing IVF cycle. The procedure itself happens entirely in the embryology laboratory; for the patient, the visible part is the IVF cycle up to egg retrieval. A Cloudnine fertility specialist and embryologist will walk you through the exact sequence used at your centre, but the broad steps are consistent.
Hormonal injections are used for roughly 10-14 days to encourage the ovaries to mature several eggs at once. Eggs are then collected under sedation through a short transvaginal procedure. This part of the cycle is identical regardless of whether you plan a fresh transfer, a frozen transfer, or only freezing.
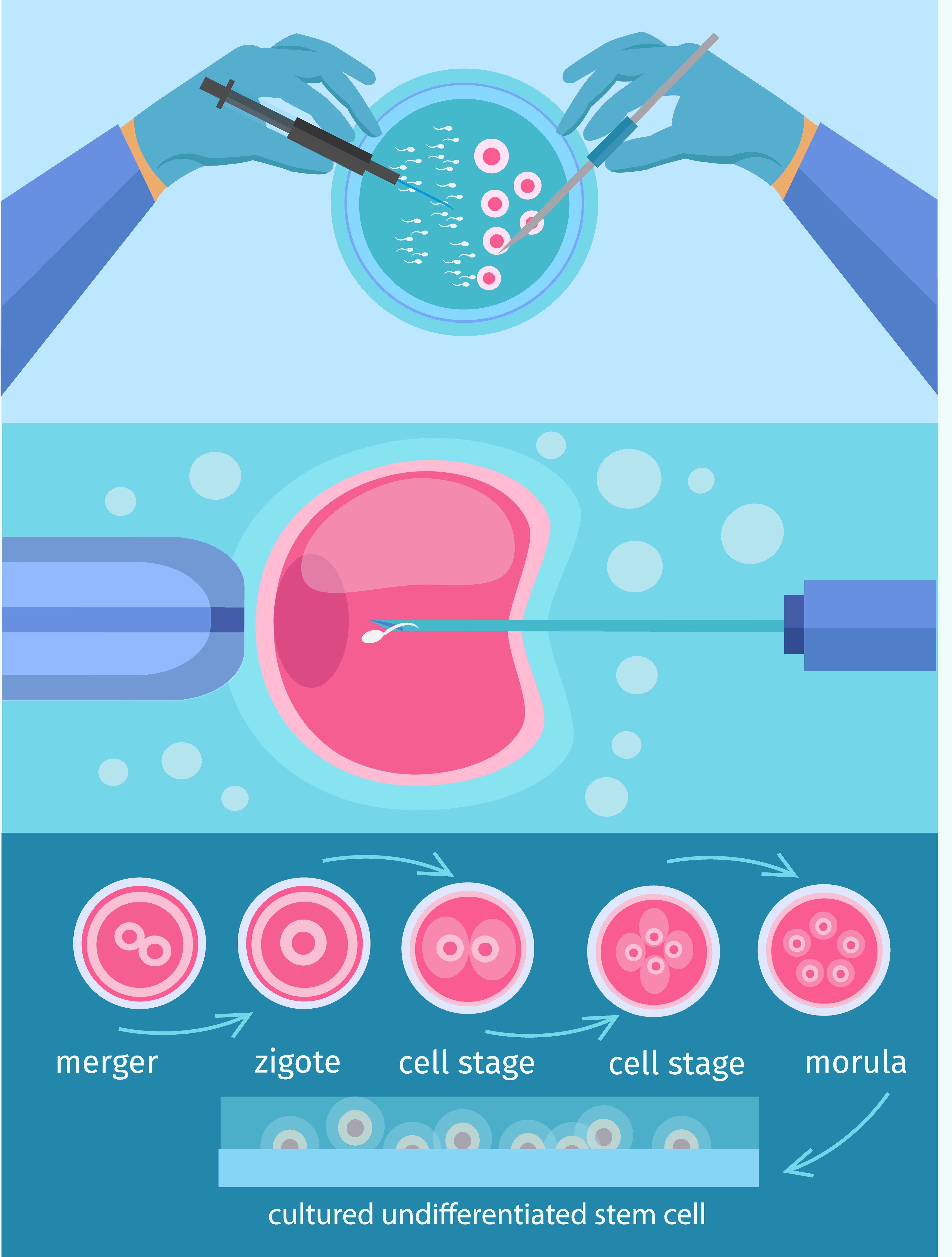
Collected eggs are fertilised in the laboratory, either through conventional IVF or by ICSI (intracytoplasmic sperm injection, used when sperm parameters require it). Resulting embryos are then cultured in carefully controlled incubators for 5-6 days until they reach the blastocyst stage, when the inner cells (which become the baby) and outer cells (which become the placenta) are clearly differentiated.
Before freezing, each blastocyst is graded by the embryologist on three parameters: expansion (how developed the blastocyst is, scored 1–6), inner cell mass quality (graded A, B or C), and trophectoderm quality (also graded A, B, or C). A 4AA, 4AB, or 5AA blastocyst is generally considered top quality, while a 3BB or 4BC may still be perfectly viable. The grade influences priority for transfer but does not automatically exclude lower-graded embryos from being frozen, as many of these still result in healthy pregnancies.
Each chosen blastocyst is exposed briefly to a cryoprotectant solution that draws water out of the cells and replaces it with substances that protect against ice damage. The embryo is then placed on a fine carrier (a vitrification straw) and plunged into liquid nitrogen at -196 °C. Cooling happens at thousands of degrees per minute, fast enough that water has no time to crystallise. Each straw is labelled with a unique identifier linking it to the patient's records.
Vitrified embryos are stored in cryogenic tanks within the embryology laboratory. At Cloudnine Fertility-grade centres, tanks are continuously temperature-monitored with alarms, and nitrogen levels are checked and topped up according to a strict schedule. Embryos can remain viable in this state for many years - and pregnancies from embryos frozen for over a decade have been reported in published case series - with no measurable decline in quality.
When you return for transfer, the chosen embryo is warmed rapidly, the cryoprotectant is washed out in graded steps, and the embryo is assessed for survival. A modern vitrification programme typically reports survival rates above 95%. The embryo is then transferred into the uterus during a frozen embryo transfer (FET) cycle, in which your endometrium (the lining of the uterus) is carefully prepared with hormonal support so that the timing matches the embryo's stage of development.
Embryo freezing is not just a backup - for many couples, it is the preferred plan. The most common reasons a Cloudnine fertility specialist will recommend freezing one or more embryos include:

Embryo freezing involves clinical, financial, and emotional decisions. The most useful questions to take into your consultation at Cloudnine Fertility include:
Once your treatment plan is confirmed, day-to-day preparation is largely the same as any IVF cycle:
Embryo cryopreservation is not the right choice for every patient or every cycle. The following situations are common reasons to ask a Cloudnine Fertility specialist whether freezing should be part of your plan.
If any of these apply to you, book a fertility consultation with a Cloudnine specialist to discuss whether embryo freezing fits your situation.

Outcomes from cryopreservation are best understood in two stages: how well embryos survive thawing and how many result in a healthy pregnancy. The numbers below are typical ranges reported in published cohorts and Indian centre audits; your own results depend on age, embryo grade, and uterine factors. A Cloudnine specialist will personalise these figures during counselling.

