A normal ovary in a woman of reproductive age measures roughly 30 mm long, 25 mm wide, and 15 mm thick (about 3 × 2.5 × 1.5 cm), with a volume of around 5-10 cc. Ovary size within this range supports natural conception, but slightly smaller or larger ovaries can still result in pregnancy if ovulation and hormone levels are normal.
Normal Ovary Size: The mm Chart
Ovary size is measured on a transvaginal ultrasound (an internal pelvic scan) and reported as length × width × thickness in millimetres or centimetres. Volume is calculated in cubic centimetres (cc) or millilitres (mL) - the two are the same. The chart below shows the size range that fertility specialists treat as normal for a healthy adult ovary.
Book an online appointment with Dr. Arockia for any fertility issues
Measurement
Normal range (mm)
Normal range (cm)
Volume (cc)
Length
25-50 mm
2.5-5.0 cm
-
Width
15-30 mm
1.5-3.0 cm
-
Thickness
10-20 mm
1.0-2.0 cm
-
Average size
30 × 25 × 15 mm
3.0 × 2.5 × 1.5 cm
5-10 cc
Full normal volume range
-
-
0.8-12.7 cc
Both ovaries are not always the same size. A 1-5 mm difference between the right and left ovary is normal and is not, on its own, a fertility problem. What matters more is whether each ovary is producing follicles and ovulating.
Why Ovary Size Matters When Trying to Conceive
For couples trying to get pregnant in Gurgaon, Delhi NCR, and beyond, ovary size is often the first finding mentioned on a pelvic ultrasound report - and it usually causes more anxiety than it should. Size is a clue, not a verdict. A normally sized ovary suggests a healthy ovarian reserve (your remaining egg supply) and an environment where follicles can grow and release eggs each cycle. Significantly smaller ovaries can point to diminished reserve or premature ovarian insufficiency, while significantly larger ovaries can point to PCOS (polycystic ovary syndrome), cysts, or an over-response to fertility medication. The number alone does not predict pregnancy - but it does tell your specialist where to look next.
Is Ovary Size Important to Get Pregnant? The Honest Answer
Yes, ovary size is important - but it is not the only thing that decides whether you can conceive. Specialists use ovary size alongside ovarian reserve markers, ovulation patterns, hormone levels, fallopian tube health, and your age. The sections below explain how size connects to pregnancy chances in real clinical practice.
Right vs left ovary: do both need to be the same size?
No. The right and left ovaries often differ slightly, and this is normal. Many women have one slightly larger ovary that does most of the ovulating in a given cycle, while the other rests. As long as both ovaries are within the normal range and at least one is producing mature follicles, natural conception is possible. A persistent, large size difference (one ovary much bigger than the other) is worth investigating, because it can suggest a cyst, endometrioma, or a structural issue.
Ovary size by age: why it changes through life
Ovaries are not the same size at every life stage. They grow during puberty, reach their full adult size during the reproductive years, and shrink after menopause as the egg supply runs down. The chart below shows the typical pattern.
Life stage
Typical ovarian volume
What it usually means for fertility
Childhood (before puberty)
Less than 1 cc
Not yet active; no ovulation
Puberty to early 20s
3-6 cc
Peak fertility years, strong ovarian reserve
Mid-20s to early 30s
5-10 cc
Reproductive prime, regular ovulation expected
Mid-30s to early 40s
3-6 cc
Reserve gradually declining; size starts to reduce
Perimenopause
1-3 cc
Cycles are becoming irregular; lower egg supply
Postmenopause
Less than 2 cc
Ovulation has stopped
Ovary size by cycle phase: why your scan timing matters
Ovary size is not fixed across the month. A scan done on Day 8, when a dominant follicle is growing, will show a larger ovary than a scan on Day 2. If your ultrasound report flags a bigger ovary, the cycle day matters: a 4-5 cc difference between an early-cycle and a mid-cycle scan is expected, not abnormal. This is one reason fertility specialists prefer baseline scans on Day 2 or Day 3 of your period, when the ovaries are at rest.
When the ovary size genuinely affects pregnancy chances
Size does start to matter when it falls outside the normal range and is paired with other findings. Smaller-than-normal ovaries with low AMH (anti-Müllerian hormone - a blood marker of egg supply) and a low antral follicle count point to diminished ovarian reserve, where fewer eggs are available each cycle. Larger-than-normal ovaries with many small follicles, irregular periods, and high LH (luteinising hormone) point to PCOS, where many follicles start, but none mature. In both cases, ovary size is a signal, not the diagnosis on its own.
What Causes Ovaries to Be Smaller or Larger Than Normal
Ovary size is influenced by hormones, age, and underlying conditions. The most common reasons your specialist will look for include:
Age and natural ovarian ageing: ovaries shrink gradually from the mid-30s as the egg supply declines.
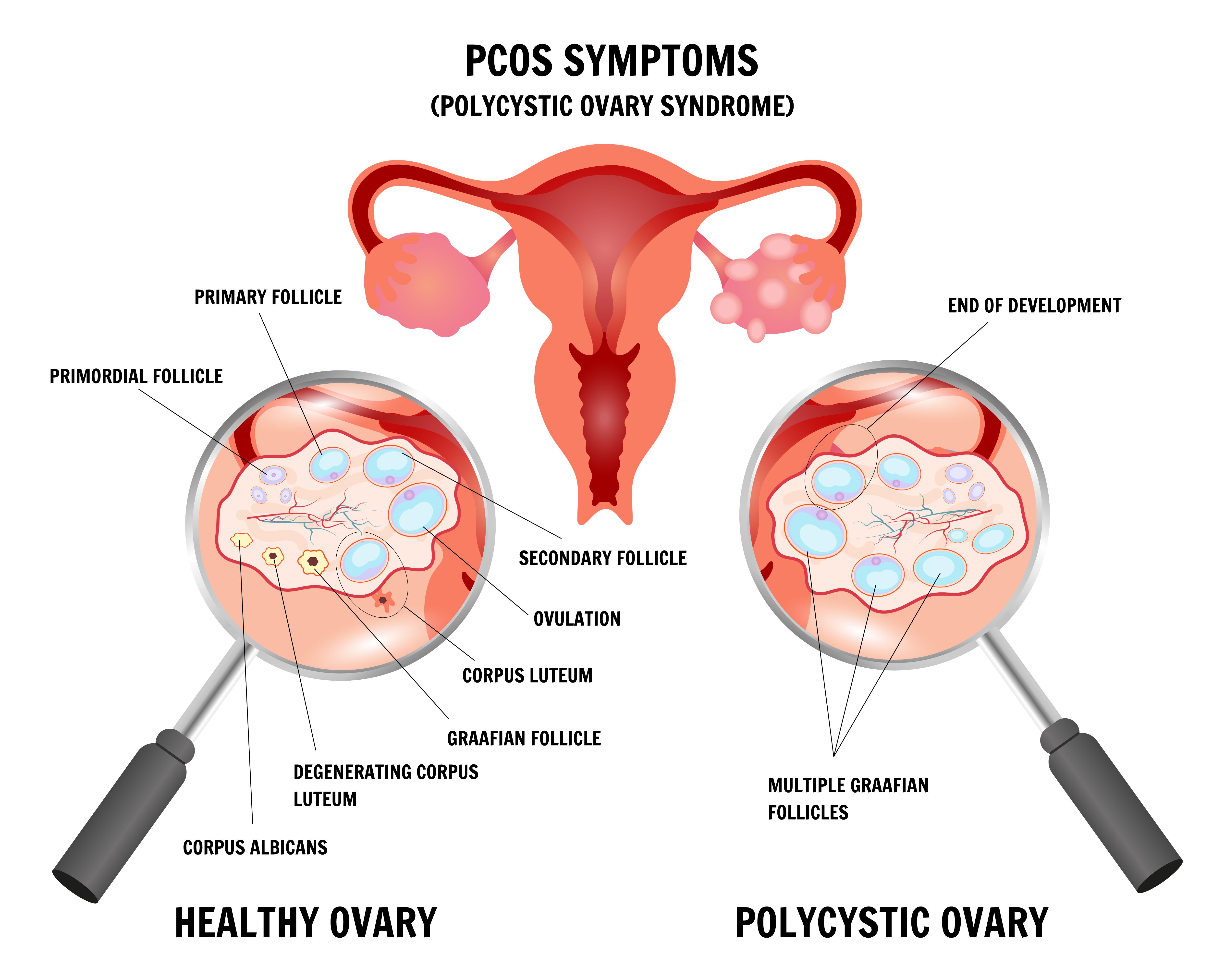
PCOS (polycystic ovary syndrome): classically causes both ovaries to be enlarged with 12 or more small follicles (2-9 mm) and a volume above 10 cc.
Diminished ovarian reserve: smaller ovaries paired with low AMH and a low antral follicle count.
Premature ovarian insufficiency (POI): ovaries become small and inactive before age 40.
Ovarian cysts and endometriomas: can temporarily enlarge one ovary, often asymmetrically.
Ovulation induction or IVF stimulation: fertility medication can temporarily push the ovaries to 6-10 cm during a treatment cycle.
Previous ovarian surgery: removal of cysts, endometriomas, or part of the ovary can permanently reduce its size.
Pelvic infection or radiation can damage ovarian tissue and reduce its size
What to Do if Your Ovary Size is Not Normal
Steps you can take at home
Lifestyle does not directly change ovary size, but it does support the hormonal environment in which your ovaries work. Helpful starting points:
Track your cycle for at least three months - note period dates, length, and any mid-cycle symptoms - so your specialist can spot patterns.
Aim for a stable, balanced eating pattern with adequate protein, whole grains, healthy fats, and vegetables; sudden weight loss or very low-calorie diets can disrupt ovulation.
Move regularly with moderate activity such as walking, yoga, or swimming, while avoiding extreme exercise if your cycles have become irregular.
Prioritise sleep and stress management, since both directly affect the brain-ovary hormonal axis.
Limit smoking and heavy alcohol use, both linked to lower ovarian reserve and earlier ovarian ageing.
Discuss any supplements, such as folic acid or vitamin D, with your fertility specialist before starting them, rather than self-prescribing.
Steps your fertility specialist may take
If a scan shows your ovaries are smaller or larger than expected, a Cloudnine specialist will usually begin with a focused evaluation:
Repeat ultrasound on Day 2 or Day 3 of your cycle to get a clean baseline measurement of both ovaries.
Antral follicle count to see how many resting follicles are visible at the start of the cycle.
Blood tests - AMH, FSH, LH, TSH, prolactin, and estradiol - to map your hormonal picture.
Targeted treatment for the underlying cause: PCOS management, ovulation induction, or IVF planning, where appropriate.
Ovarian reserve discussion if you are over 35, planning to delay pregnancy, or have a family history of early menopause.
When to See a Fertility Specialist
Your situation
Recommended action
Under 35 and trying for 12 months without conception
Book a fertility evaluation
35 or older and trying for 6 months without conception
Book a fertility evaluation now
Ultrasound has flagged the ovary size as small, large, or asymmetric
Confirm with a baseline Day 2/3 scan and ovarian reserve testing
Cycles consistently shorter than 21 days or longer than 35 days
See a specialist regardless of how long you have been trying
Known PCOS, endometriosis, thyroid disorder, or previous ovarian surgery
See a specialist before you start trying, if possible
No periods for 3 months or more (and not pregnant)
See a specialist promptly
Family history of early menopause or premature ovarian insufficiency
Discuss ovarian reserve testing early
If any of these apply, you can book a fertility consultation with a Cloudnine Fertility specialist to assess your ovary size, ovarian reserve, and next steps.
How Ovary Size Translates Into Pregnancy Outlook
Ovary size is interpreted alongside ovarian reserve markers and ovulation. The table below shows how typical findings are usually read in practice.
Ultrasound finding
What it usually means
Typical implication for pregnancy
Both ovaries 3-10 cc, regular ovulation
Normal reproductive picture
Natural conception likely; standard timed approach
Ovaries less than 3 cc with low AMH
Diminished ovarian reserve
Reduced egg supply; earlier intervention is often advised
Ovaries above 10 cc with 12+ small follicles
Suggests PCOS
Ovulation is often irregular; treatable with lifestyle and ovulation induction
One ovary much larger than the other
Possible cyst, endometrioma, or structural issue
Needs targeted evaluation; usually treatable
Ovaries less than 2 cc with very high FSH
Premature ovarian insufficiency
Donor egg or specialised IVF pathway is often discussed
Ovaries enlarged after fertility medication
Expected stimulation response
Usually resolves; monitored to avoid hyperstimulation
Want to consult the best fertility in india? Please find the links below.